Endobronchial Stenting: Restoring Airway Patency with Precision and Innovation
Introduction
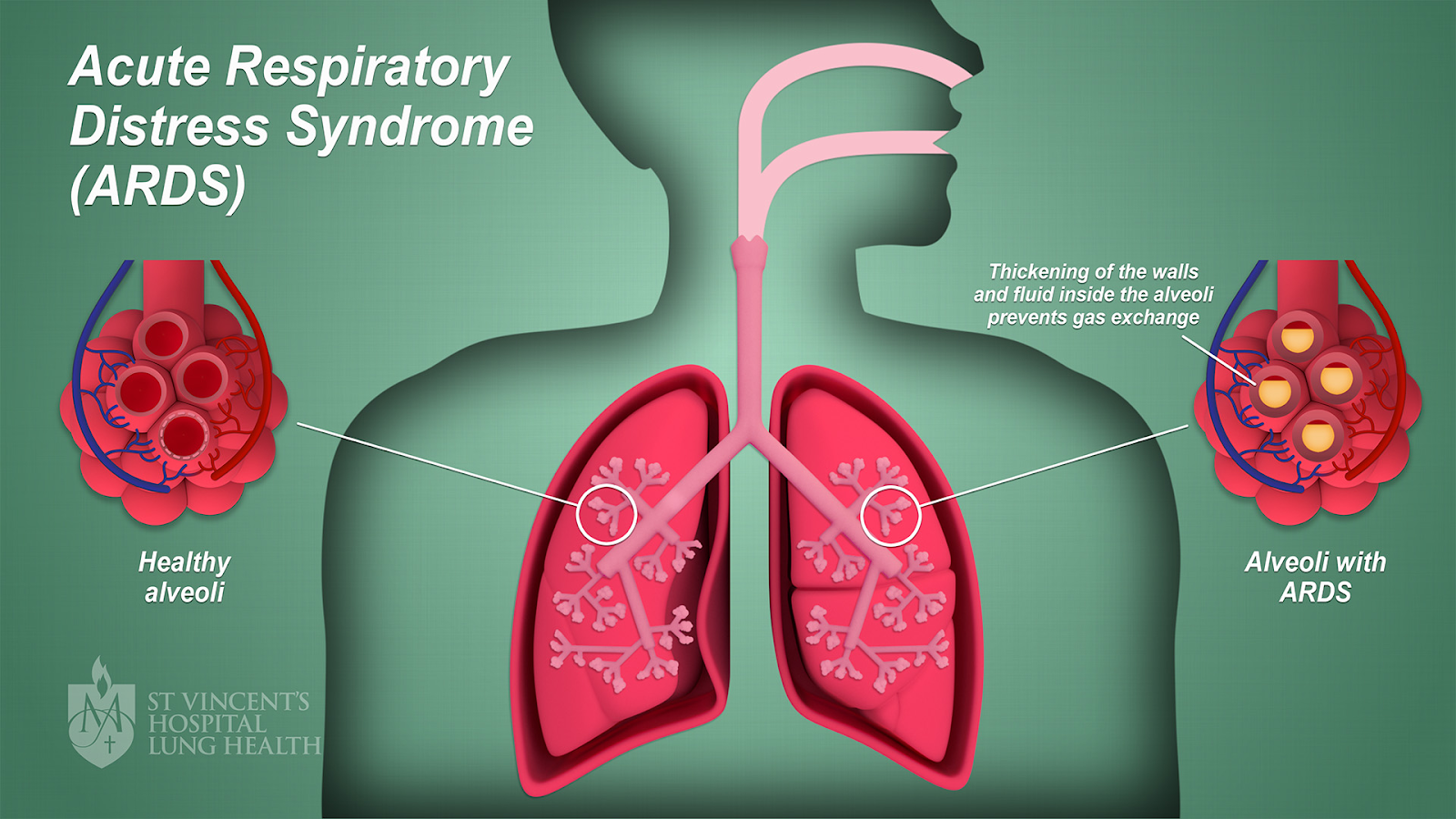
Endobronchial stenting has emerged as a pivotal intervention in managing various airway pathologies, particularly those leading to central airway obstruction (CAO). This procedure involves the placement of a stent within the tracheobronchial tree to maintain airway patency, thereby alleviating symptoms and improving the quality of life for affected patients. This comprehensive overview delves into the indications, types, techniques, outcomes, and potential complications associated with endobronchial stenting, with a focus on literature from 2021 to 2025.
 |
| image credit |
Indications for Endobronchial Stenting
Endobronchial stenting is primarily indicated in scenarios where airway patency is compromised. The main indications include:
Malignant Airway Obstruction: Tumors originating from the trachea or bronchi, or metastatic lesions causing extrinsic compression, can lead to significant airway narrowing. Stenting serves as a palliative measure to relieve obstruction and improve ventilation.
Benign Airway Stenosis: Conditions such as post-intubation tracheal stenosis, inflammatory diseases, or congenital anomalies can result in benign strictures. While surgical resection remains the definitive treatment, stenting offers a less invasive alternative, especially in patients unfit for surgery.
Tracheoesophageal and Bronchopleural Fistulas: Abnormal communications between the trachea and esophagus or pleural space can lead to severe respiratory complications. Stent placement helps seal these fistulas, preventing aspiration and improving respiratory function.
- Airway Collapse Due to Extrinsic Compression: Mediastinal masses or lymphadenopathy can exert pressure on the airway, leading to collapse. Stenting provides structural support, counteracting the external compressive forces.
 |
| image credit |
Types of Endobronchial Stents
The selection of an appropriate stent is crucial and depends on the underlying pathology, anatomical considerations, and the desired duration of stenting. The primary types include:
1. Silicone Stents
Silicone stents have been widely used in the treatment of both benign and malignant airway obstructions. They are typically inserted using a rigid bronchoscope and provide a non-reactive, biocompatible solution for maintaining airway patency.
Advantages
✅ Biocompatibility: Made of medical-grade silicone, reducing inflammation and tissue reaction.
✅ Easy Removal: Unlike metallic stents, silicone stents can be safely removed, making them ideal for temporary airway management.
✅ Lower Risk of Granulation Tissue Formation: Since they do not embed into the airway wall, the risk of excessive tissue overgrowth is lower.
✅ Customizable: Available in various sizes and shapes; some can be trimmed to fit individual patient anatomy.
Disadvantages
❌ Migration Risk: More prone to displacement, especially in mobile airway regions like the trachea.
❌ Mucus Plugging: Their non-porous surface can accumulate secretions, leading to obstruction.
❌ Rigid Bronchoscopy Requirement: Placement often requires general anesthesia and specialized equipment.
❌ Limited Radial Force: Less effective for extrinsic airway compression compared to metallic stents.
Best Used For
- Benign airway stenosis (e.g., post-intubation tracheal stenosis).
- Airway fistula sealing (e.g., tracheoesophageal fistulas).
- Patients requiring temporary stenting with an option for removal.
 |
| The original Dumon Stent (Tracheobronxane ®, Novatech, la Ciotat, France) image credit |
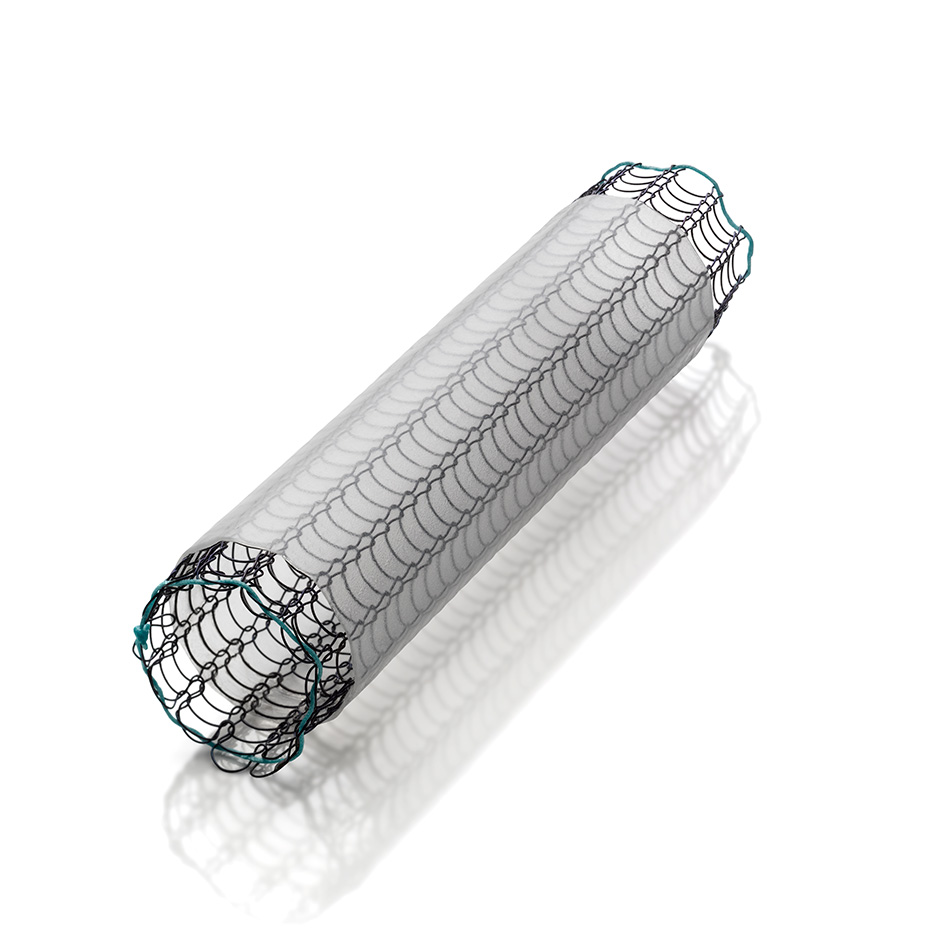
2. Metallic Stents (Self-Expanding and Balloon-Expandable)
Metallic stents, also known as self-expanding metal stents (SEMS), are widely used for malignant airway obstructions due to their excellent radial force and ability to resist external compression. These stents are usually composed of nitinol (nickel-titanium alloy), stainless steel, or cobalt-chromium and are inserted via a flexible bronchoscope.
Types of Metallic Stents
- Self-Expanding Metallic Stents (SEMS) – Expand upon deployment, commonly used in malignant obstructions.
- Balloon-Expandable Stents – Require external balloon dilation for expansion, used in certain rigid airway obstructions.
Advantages
✅ Strong Radial Force: Ideal for relieving extrinsic compression from tumors or lymphadenopathy.
✅ Minimally Invasive: Can be placed using flexible bronchoscopy under sedation.
✅ Lower Migration Rate: Compared to silicone stents, they stay in place better.
✅ Thin-Walled Structure: Provides a larger airway lumen than silicone stents of the same outer diameter.
Disadvantages
❌ Difficult Removal: Tends to embed into the airway wall, making removal challenging and sometimes requiring surgery.
❌ Granulation Tissue Formation: Chronic irritation leads to tissue overgrowth, potentially causing re-obstruction.
❌ Fracture Risk: Over time, metal fatigue can lead to stent fracture.
❌ Foreign Body Reaction: Some patients may experience chronic inflammation.
Best Used For
- Malignant airway obstruction (e.g., lung cancer, tracheal tumors).
- Tracheobronchial collapse due to external compression (e.g., mediastinal masses).
- Patients with a poor prognosis where stent removal is not anticipated.
 |
| image credit |
3. Hybrid Stents (Metallic Framework with Silicone Covering)
Hybrid stents combine the benefits of both metallic and silicone stents. They have a metallic framework for radial strength but are coated with silicone to reduce tissue ingrowth and facilitate removal.
Advantages
✅ Lower Granulation Tissue Formation: The silicone covering reduces direct metal-to-tissue contact.
✅ Strong Radial Force: Offers better airway support than pure silicone stents.
✅ Reduced Migration Risk: More stable than traditional silicone stents.
✅ Easier Removal: Can be extracted more easily than bare metallic stents.
Disadvantages
❌ Potential Mucus Plugging: The silicone coating can lead to secretion accumulation.
❌ Limited Flexibility: May not conform as well to highly distorted airways.
❌ Higher Cost: More expensive than conventional silicone or metallic stents.
Best Used For
- Malignant or benign airway obstruction requiring long-term management.
- Patients needing a balance between structural support and removability.
- Cases where granulation tissue formation needs to be minimized.
Comparison Table: Stent Types at a Glance
| Feature | Silicone Stents | Metallic Stents (SEMS) | Hybrid Stents |
|---|---|---|---|
| Material | Medical-grade silicone | Nitinol, stainless steel | Metal framework with silicone coating |
| Placement | Rigid bronchoscopy | Flexible bronchoscopy | Flexible or rigid bronchoscopy |
| Radial Force | Low | High | Moderate to high |
| Migration Risk | High | Low | Moderate |
| Granulation Tissue Formation | Low | High | Lower than metal stents |
| Secretion Accumulation | High | Low | Moderate |
| Ease of Removal | Easy | Difficult | Easier than metallic stents |
| Best For | Benign conditions, temporary airway support | Malignant obstruction, external compression | Long-term airway support with removability option |
Emerging Trends and Future Developments
The field of airway stenting is evolving, with new technologies aimed at improving stent performance and minimizing complications:
3D-Printed Stents
- Custom-made stents tailored to patient-specific airway anatomy.
- Expected to reduce migration risk and improve patient outcomes.
Biodegradable Stents
- Designed to degrade over time, eliminating the need for removal.
- Particularly useful for temporary airway support in benign conditions.
Drug-Eluting Stents
- Coated with anti-inflammatory or antibiotic agents to reduce granulation tissue formation and infections.
- May improve long-term outcomes in patients with chronic airway disease.
Techniques of Stent Placement
Pre-procedural Assessment: Comprehensive evaluation includes imaging studies like computed tomography (CT) scans to delineate the anatomy and extent of obstruction. Pulmonary function tests may also be conducted to assess the baseline respiratory status.
Bronchoscopic Guidance: The procedure is typically performed under general anesthesia using flexible or rigid bronchoscopy. The choice depends on the stent type and the specific clinical scenario.
Fluoroscopic Assistance: Real-time fluoroscopy aids in accurate stent deployment, ensuring proper positioning and expansion.
Post-deployment Evaluation: After placement, bronchoscopy is repeated to confirm stent position and assess for any immediate complications such as bleeding or misplacement.
Outcomes and Efficacy
The success of endobronchial stenting is measured by symptom relief, improvement in airway patency, and quality of life enhancements:
Symptomatic Improvement: Patients often experience immediate relief from dyspnea and other respiratory symptoms post-stenting.
Enhanced Airway Patency: Imaging and bronchoscopic evaluations post-procedure typically show significant improvement in airway diameter.
Quality of Life: Studies have reported improved quality of life scores in patients undergoing stenting for malignant obstructions, with reduced need for additional interventions.ns and Management
While endobronchial stenting is generally safe, potential complications can arise:
Stent Migration: More common with silicone stents, migration can lead to recurrent obstruction or airway injury. Securing the stent adequately during placement and selecting the appropriate size can mitigate this risk.
Granulation Tissue Formation: Particularly associated with metallic stents, excessive tissue growth can re-occlude the airway. Regular bronchoscopic surveillance and, if necessary, interventions like laser therapy can manage this complication.
Infection: The presence of a foreign body can predispose to infections. Prophylactic antibiotics and ensuring optimal stent hygiene are preventive strategies.
Mucus Plugging: Stents can act as a nidus for mucus accumulation, leading to obstruction. Nebulized mucolytics and adequate hydration are recommended to prevent this issue.
Recent Advances and Future Directions
The field of endobronchial stenting is continually evolving:
3D-Printed Stents: Custom-made stents tailored to individual patient anatomy using 3D printing technology are being explored, promising better fit and reduced complications.
Biodegradable Stents: Research is ongoing into stents that gradually degrade over time, potentially reducing the need for removal procedures and minimizing long-term complications.
Drug-Eluting Stents: Incorporating medications such as anti-inflammatory agents or antibiotics into the stent material aims to prevent complications like granulation tissue formation and infections.
Conclusion
Endobronchial stenting remains a vital tool in the management of various airway pathologies, offering significant symptomatic relief and improved quality of life for patients with airway obstructions. Ongoing research and technological advancements continue to refine stent designs and placement techniques, aiming to enhance efficacy and safety. As with any medical intervention, careful patient selection, meticulous procedural execution, and diligent post-procedural care are paramount to achieving optimal outcomes.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}